By: Michael J. Rice Ph.D., ARNP. BC.
Michael has been employed by the Washington
State College of Nursing, Spokane Washington since
1989. An associate professor, he teaches in the Psychiatric
Nurse Practitioner Program. He received his Master's Degree
in Psychiatric Nursing from the College
of Nursing at the University of Nebraska Medical Center,
Omaha Nebraska in 1976. He received his PH.D in Clinical
Nursing Research from the University
of Arizona College of Nursing in 1988. He has been
board certified by ANCC in Psychiatric Mental Health since
1995 and is licensed as a Psychiatric ARNP in Washington
State. He also has a private practice at the Suncrest
Wellness Center which is located in Steven's County
Washington, a federally designated medically underserved
rural community. He is a strong advocate for the use of
technology to meet health care needs in rural communities
and the recipient of the prestigious EDUCAUSE 2002 Award for Excellence in Technology Solutions.
|
|
By: Ryan Townsend, MN, ARNP, BC
Ryan currently holds a faculty position at Washington State University College of Nursing working with undergraduate students in class and clinical instruction. Ryan received his Master's Degree at Washington State University College of Nursing in 2004. While in his Master's program he served as research assistant for the Medically Indigent Rural Area (MIRA) Psychiatric Nurse Practitioner Program at Washington State University. He is a practiticing Psychiatric Mental Health Nurse Practitioner who currently works at the People's Clinic of Spokane and in his own private practice both in Washington.
|
|
April 12 2006
In the Pacific Northwest one nursing institution utilizes PDAs in the Masters of Nursing Psychiatric/ Mental Health Nurse Practitioner Program (PMHNP). Throughout the program, the PDAs were used to schedule patients, access drug information, document patient findings and track personal tasks. Partially funded by a grant from Suffolk Community College and Symbol Technologies this study examined the frequency of PDA stress experiences in a nurse clinical practicum.
Literature Review
PDA literature indicates usage is increasing within the healthcare professions because the PDA is valuable tool. Reports state that the PDA is valued for its mobility and the wealth of data that can be accessed by providers at the point of care for patients (Fontelo, Ackerman, & Locatis, 2003; Chin, 2000; Martinez de Castro, 1997). The literature also supports decreases in medication error rates and adverse drug events due to PDA utilization (Wilcox & La Tella, 2001; Grasso,& Genest 2001). Studies indicate that PDA’s can ease the provider burden in scheduling, billing, and overall communication (Blackman, Gorman, Lahensohn, Kraemer, & Svingen, 1999). PDA’s can maintain security and confidentiality which is important in the healthcare arena (Duncan & Shabot, 2000). Wilcox and LaTella (2001) argue that PDAs will become to providers as important as the stethoscope in terms of providing care.
The literature argues for educational use of PDA technology in healthcare learning environments. Rice (2003, ¶ 1) when addressing PDAs and deficits in care in rural areas stated:
“The advent of the Personal Digital Assistants and their use in health care possess the potential for resolving many of these resource problems. Yet, health care professionals’ familiarity with the PDA’s must begin in their educational programs.”
In support of this need for familiarity with PDA’s in educational programs the National League for Nursing (2002) “made ““infusing technology into concepts, structures, and processes of nursing education”” one of the nursing education research priorities to ensure nursing graduates’ competency for the 21st century” (McCannon & O’Neal, 2003, p. 338). This position by the National League of Nursing supports use of new technologies in the PMHNP program.
Significance
There is limited nursing knowledge on the usage of educational technologies and the resulting student stress. The impact of stress of PDAs needs to be assessed due to the negative effects of stress on learning (McEwen, 2000). Currently, there is sparse information on the stress associated with educational technology in the form of PDAs. Once the frequency of stress has been identified, future research will then be able to focus on interventions to reduce the negative effects of stress on learning and support the educational process. This information on stress occurrence and PDA utilization could further the use and implementation of this technology more fluidly in the educational setting with minimal impact on students.
Setting for Study
The settings for this study included the rural and medically underserved clinical sites where the graduate students used the PDAs in their practicum and internship clinical courses. Over seventy percent of these sites are located in rural and medically underserved areas which extended over 100,000 square miles (Rice, 2003). Medically underserved areas lack healthcare provider service (Rice, n.d.). The goal of the nursing college in this study is to increase the number of PMHNPs who reside in rural underserved areas (Rice n.d.). The lack of educational support is managed with distance educational technologies. The purpose of the PDA implementation was to add another valuable tool to aid providers in fulfilling the gap in underserved areas.
Evaluating the stress involved in adapting to the use of new technology in locations within the study setting the used the “Stress of Educational PDA Technology” scale available on the web. The web site was available for students and hard copies of the scale were mailed to students at study sites as well. Thus, students in far flung rural areas, often more than 100 miles from the main campus, could answer the scale anywhere they could log on to the web site.
Population and Sample
The sample available for this study was the graduate students at the nursing college in the PMHNP program in their advanced practicum and internship clinical experiences.
Sample Criteria
The sample met the following criteria:
- were 21 and older,
- included males or females,
- included all ethnic backgrounds, and
- no restrictions were placed on income, current job classification, or race or setting of clinical experience. Inclusion criteria also included that the student was in the graduate program. All participants had to be in the practicum phase or internship courses in the PMHNP curriculum.
Instrumentation: Reliability and Validity
In order to measure the stress of PDA utilization, a scale needed to be developed due to the lack of identification of a preexisting scale. The “Stress of Educational PDA Technology” scale is a highly modified stress scale originally designed by Horowitz (1979) to measure traumatic stress responses. Approval was given to use this scale by Horowitz. This scale was then modified for this investigation to gauge the level of stress associated with using PDA educational technology. The reliability of this scale was unknown prior to this study as it was a new scale.
The original stress scale by Horowitz had 15 items. However, as one of the items did not have relevant face validity for this investigation, “The Stress of Educational PDA Technology” scale was modified to 14 items. Each of the 14 items were altered to address the issues of stress response to using PDAs. The scale asks students to rate their perception with values ranging from 0-five points using a Likert type scale. Answers indicating more stress are given a value of 5 and conversely answers that indicate no stress are given a value of zero. The values are then totaled for all items on the scale.
Human Subjects Consideration
Informed consent was approved by the WSU-IRB and was given to each participant prior to study enrollment for the parent study. An amendment approved by the IRB allowed for “The Stress of Educational PDA Technology” scale. Participants could ask questions prior to enrollment. Signed consent pages were collected by the primary investigator and filed with the parent study.
Results
Sample demographics of thirteen subjects were collected separate from the scale data. The sample was 76.9% female and 23.1% male. About half of the sample (53.8%) was age 40-49. 23.1% of the sample were 30-39 years old and 23.1% were 50-59 years old. The sample lived in both urban and remote site campuses. A total of 61.5% of the sample utilized the main campus and 38.5% utilized outreach program sites. Five responders reported completing the stress survey during the first third of the semester and 80% perceived their computer ability as intermediate, 20% stated they were experts.
Scale Reliability
“The Stress of Educational PDA Technology” scale was analyzed using SPSS and Crohnbach’s alpha. The breakdown of scores for this study comprised of three total scale scores below 8, five scores in the 9-25 range, and five scores greater than 26. The highest score was a 45 and the lowest score was zero. The average score for all of the students was 21.5. Analysis of the data indicated that the Crohnbach’s alpha was .76. The reliability estimate of .76 indicated that the scale had a strong level of internal consistency for a new scale.
Frequency of Stress Responses
The analysis of the data indicated that there were some variances in the student responses. Several of the students felt that the PDAs interfered with their learning. Almost half, (46.2 percent) of the subjects provided answers that ranged from “rarely,” “sometimes,” or “often” about feelings that the stress of using the PDA devices interfered with their learning
(Figure 1).
Figure 1: Bar Graph on “The stress of using my PDA interferes with my learning.”
The scale determined that 46.2 percent of subjects became upset when they thought about using the PDA (Figure 2).
Figure 2: Bar Graph on “I got upset when I thought about using my PDA.”
Also 53.8 percent of subjects felt some degree of being overwhelmed by their feelings about PDA usage (Figure 3).
Figure 3: Bar Graph on “I was overwhelmed by my feelings of PDA usage.”
Non stressed Students
While approximately half of the subjects had problems with the use of the PDAs, a significant percentage of the subjects were not stressed with the use of the PDAs. Analysis of Figures 1-2, indicate that greater than 50% of the subjects were not bothered at all by the adaptation of the PDAs. This subset of the sample consistently reported comfort in the use of the PDAs. As indicated in Figure 4, 46.2% of subjects were not overwhelmed with the use of PDAs. However, in Figure 6, the percent that were not distressed by the use of the PDAs dropped to 38.5%, but this was still a large section of the population.
Figure 4: Bar graph on “I was overwhelmed by my feelings of PDA usage.”
Figure 5:Bar graph on “I tried to talk about the PDA use to get more comfortable.”
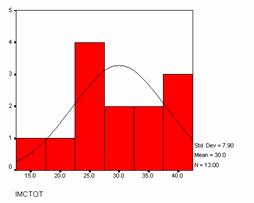
The data identified that there were clearly two sets of individuals in this study. The sample was composed of one group not displaying a stress response in adapting to PDA technology and one group that did display a response. This is best represented in Figure 6, which is the sum of scale answers plotted on a bell curve. The size of these two groups is almost equal as indicated by the graph.
Figure 6: The sum of scale answers plotted on a bell curve.
Relationships Between Feelings
Relationships between the variables were analyzed using Pearson’s correlations. Strong relationships above .7 were found to exist among scale items that indicate a negative level of stress. An example would be the scale item “I got upset when I thought about using my PDA” and the scale item “the stress of using my PDA interferes with my learning” had a .974 correlation (p=.001). However, the same scale item “I got upset when I thought about using my PDA” had weak correlation with positive scale items such as “I had thoughts on how to use PDA in clinical” resulting in an insignificant correlation. The correlations generally indicated consistently strong relationships between items that reflect negative levels of stress. The analysis indicted that those who had stress consistently had stressful responses through out the use of the PDAs.
Discussion and Implications
A review of the existing literature, both on computer anxiety and the increased importance of PDAs in clinical care, highlights the importance of this investigation. Stress negatively impacts learning and there is good support that computers produce anxiety for a portion of the population (McEwen, 2000; McEwen 2003; Gos, 1996; Orr, n.d.). It is important to identify the stress associated with micro computers, like PDAs, which have become increasingly common in educational settings.
The results of this study indicate that approximately 50 percent of the subjects experience a significant amount of stress when beginning to use PDAs for educational purposes. These results were generated from a sample group that could be considered technologically savvy given the environmental emphasis on technology in the nursing college. The findings on the level of stress in this investigation exceed the rate of stress reported by Orr (n.d.). Yet these findings in a technologically sophisticated environment may hold even more significance in technologically naïve populations.
The findings based on the “Stress of Educational Technology Scale” indicate that the scale identifies that there are two distinct populations in the study. These populations can be divided into one population that is not stressed by the use of technology, and one population that is affected in terms of a stress response to the utilization of technology. The scale presents the ability to identify these groups very clearly. The implementation of this scale prior to technology implementation may be effective in identifying those with stress so that interventions may be put in place to lessen the stress response.
Prior to this study, there had been no investigations on the level of stress caused by using PDA technology in the nursing graduate educational process. This pilot study was successful in identifying the stress associated with the implementation of new educational technology in the PMHNP students utilized. The findings of this study indicate the need to confirm the findings with a larger study. Future research should focus on interventions that may lessen the stressful impact observed in approximately 50% of this study population. These interventions may be only applicable to 50% of the students, but will ultimately facilitate the educational process of all students using sophisticated technology.
Limitations
When analyzing the limitations of the study one key limitation was the fact that study design did not connect the demographic information with the data from the scales. As a result it was not possible to search for correlations between stress responses and demographic characteristics. Also due to this study being a pilot study the sample utilized thirteen subjects. While this is an adequate sample size for a pilot study, the sample is not large enough to be generalizable to many populations.
A final, and major limitation in the study, is the environment in which the students used the PDA’s. Due to the emphasis on distance education, there are two aspects that affect their responses of the students. First, in the clinical practice arenas, 70 of all clinical sites are located in rural and medically underserved areas. This requires that the student be more self reliant, but also results in isolation from technological support. Any problems and issues associated with the use of high end technologies require the students to self manage problems.
A second element in the environment that affected the student population at the nursing college in this study is that the students are not technology “naïve.” With much of the program emphasizing distance education technologies, there are a fair percentage of the students who have never been to the main Spokane campus (Rice, 2003). This means that with the student utilization of “Whets” microwave technology, IP based videoconferencing and internet “Blackboard” courses, the students at the ICN may have a higher threshold and tolerance for stress associated with using educational technology. Thus, both the positive and negative responses to the stress associated with the PDAs found in this investigation may not reflect the stress experiences by technologically naïve populations. While the nursing college in this study has one of the largest enrollments of any Psych NP program, because of the level of progression there are not a great number of students enrolled in the final clinical courses.
References
Blackman, J., Gorman, P., Lahensohn, R., Kraemer, D., & Svingen, S. (1999). The usefulness of handheld computers in a surgical group practice, 686-90. Retrieved on April 10, 2004, from PubMed.
Chin, T. (2000). Lending doctors a hand(held). Amednews.com. Retrieved April 10, 2004,
from http://ama-assn.org/amednews/2000/09/11/tesa0911.htm.
Duncan, R.G. & Shabot, M.M. (2000). Secure remote access to a clinical data repository
using a wireless personal digital assistant (PDA). Retrieved on April 10, 2004,
from PubMed.
Fontelo, P., Ackerma, M., & Locatis, C. (2003). The PDA as a portal to knowledge sources in a
wireless setting. Telemedicine Journal and e-Health, 9(2), 141-147. Abstract retrieved
April 10, 2004, from PubMed database.
Gos, M.W. (1996). Computer anxiety and computer experience: A new look at an old
relationship. Retrieved March 8, 2004, from Lee College Web site:
http://www.lee.edu/~mgos/pub.html.
Grasso, B.C., & Genest, R. (2001). Clinical computing: Use of a personal digital assistant in
reducing medication error rates. Psychiatry Services, 52, 883-886.
Horowitz, M.J. (1979) Impact of stressful events scale. Retrieved on October 15th, 2003,
from http://www.mardihorowitz.com/works.htm.
Martinez de Castro, C. (1997).Hand held computers speed University of Florida home nursing
visits. Retrieved on April 8, 2004 from http//:www.sciencedaily.com/releases/1997/05/970512100654.htm.
McCannon, M., & O'Neal, P.V. (2003).Results of a national survey indicating
information technology skills needed by nurses at time of entry into the work
force. Journal of Nursing Education, 42(8), 337-340.
McEwen, B.S. (2003). Mood disorders and allostatic load. Society of Biological Psychiatry, 54,
200-207.
McEwen, B.S. (2000) Effects of adverse experiences for brain structure and function. Society of
Biological Psychiatry, 48, 721-731.
Orr, L.V. (n.d.) Computer anxiety. Retrieved on April 8, 2004, from the University of Southern
Maine Web site: http://www.usm.maine.edu/~com/lindap~1.htm.
Rice, M.L. (n.d.) Medically indigent/rural area psychiatric NP education (Mira project).
Retrieved on April 16, 2004, from Washigton State University ICN Web site: http://nursing.wsu.edu/mira/index.asp.
Rice, M.J. (2003). Bridging the digital divide in medically underserved areas with
PDAs. Retrieved January 7th, 2004, from http://www.pdacortex.com/rural_pdas.htm
Rice, M.J., & Elgiadi. (2003) WSUCollege of Nursing MIRA Program receives grant for PDAs. Retrieved January 7th, 2004, from http://www.pdacortex.com/WSU_Grant_PDAs.htm
Wilcox, R.A., & La Tella, R.R. (2001). The personal digital assistant: a new medical instrument for the exchange of clinical information at the point of care. Medical Journal of Australia, 175, 659-662.

